Treatment Options For Endometriosis
How Is Endometriosis Treated?
The treatment of endometriosis must always be individualized and multidisciplinary. Although it is usually a complex disease, it is a benign and transitory pathology; it disappears spontaneously with menopause. Each case is studied individually based on the 3 factors that determine the treatment of the disease:
- Patient age
- Symptom severity
- Wishes for future pregnancies
Therapeutic Treatment Options for Endometriosis
Endometriosis is usually treated through one of three therapeutic options

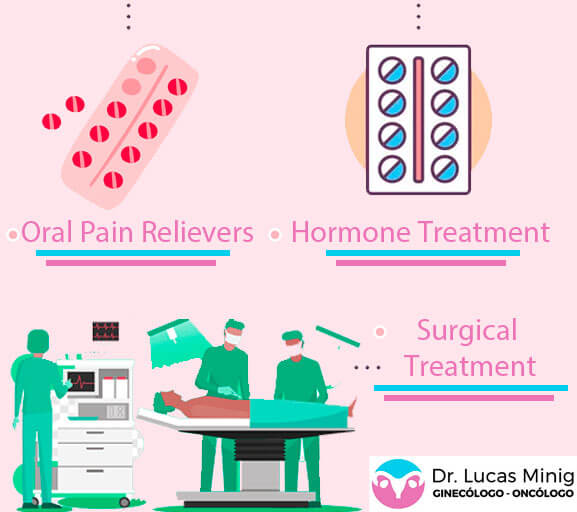
Oral Pain Relievers and Analgesics
Oral Pain Relievers are the first option for treating the symptoms of Endometriosis in mild cases. Your doctor will usually prescribe over-the-counter analgesics – anti-inflammatories such as paracetamol, dexketoprofen (Enantyum ®), ibuprofen (Advil® or Motrin®), or metamizole magnesium hexahydrate (Nolotil ®).
Hormonal Treatment:
Hormonal Treatments are usually an advantageous therapeutic option to reduce the level of pain in women and can be used in combination with analgesics.
It is important to mention that both painkillers and hormonal treatments can only be effective during their administration to manage the symptoms of Endometriosis, but they do not work to cure endometriosis entirely.
Hormonal Contraceptives & Birth Control
The goal of hormonal treatment is to suppress ovulation and, in some cases, menstruation. By doing this, it is expected that patients will reduce the severity of pain caused by endometriosis. Hormonal contraceptives can be administered orally and continuously, vaginally (ring), intrauterine (Intrauterine Devices- IUD with levonorgestrel)
There are numerous types of oral contraceptives. Those that combine estrogen and progesterone, or those with only progesterone. In any case, it is very important that contraceptives for endometriosis pain contain a specific type of progesterone: Dienogest
The most effective way to administer oral contraceptives is continuous. In other words, only the hormone pills from each box are taken, usually 21 or 24 (depending on each commercial brand). The next day, instead of taking the break (or taking the placebo pills) for 4-7 days to lower your period, you continue with the hormonal pills from the next box.
By doing this, patients will not have their period and, therefore, suppress the main cause of pain associated with endometriosis.
This method of taking contraceptives does not alter the ability of a woman to become pregnant in the future when the woman wishes to become a mother and stop taking contraceptive pills.
It is very important that the treatment is properly prescribed by a gynecologist specializing in endometriosis after a correct evaluation.
Drugs that slow down ovarian hormone production
These are gonadotropin-releasing hormone (Gn-RH) agonists and antagonists, and it is a treatment that is performed temporarily for 6 months. The objective is to stop the evolution of the disease generating a transitory menopause. It is a treatment that is used very rarely due to the adverse effects associated with transient menopause.
Surgical Treatments for Endometriosis
Surgery is the most invasive treatment option for Endometriosis, but is the most effective. In addition to having as objective to carry out the diagnostic confirmation of the presence of Endometriosis, it is also intended to remove the entirety of the diseased tissue, resulting in a significant improvement in the pain of the patients.
In certain cases of women with infertility, surgical intervention is also sought out to restore the reproductive organs to increase the possibility of pregnancy.
Only a small minority of patients with endometriosis will ultimately require surgical treatment. It is a treatment option that is used in highly selective cases when other methods of symptom management are not effective.
Today, we routinely use mini-invasive laparoscopic surgery for the surgical treatment of endometriosis in almost 100% of women who ultimately require surgical treatment of any type of complexity.
Fertility-sparing endometriosis surgery: it is the most frequently used and includes the following procedures:
- Removal of an ovarian cyst (Cystectomy)
- Removal of an ovary (Annexectomy)
- Removal of one or both fallopian tubes
- Release of pelvic adhesions: it is very common in patients with endometriosis and is one of the main causes of pain.
- Removal of superficial or deep peritoneal implants in the recto-vaginal space or bladder-ureter.
- Bowel resection: In highly selected cases of patients with infiltration of the rectum, resection of a small portion of the rectum is necessary, which is then rejoined to restore intestinal transit.
- Partial resection of the bladder and ureter: also in highly selected cases with extensive disease. The bladder is closed again and the ureter, in case it has to be sectioned, is reattached to the bladder.
- Dissection and release of pelvic nerves
Endometriosis surgery without preserving fertility: it is used in highly selected cases where the disease (and pain) progress despite all the aforementioned treatments. And it is only reserved for patients who have fulfilled their expectations of maternity or who do not want to be mothers in the future. It includes the following procedures:
- Removal of the uterus: Hysterectomy
- Removal of both ovaries: This causes surgical menopause, which is why it is used in extreme cases of uncontrollable pain.
Testimonials from patients operated on for Endometriosis in Spain
Learn about the opinions and testimonials of women who have undergone endometriosis treatment at our medical center.
Doctor Lucas Minig Specialist in the treatment of Endometriosis in Valencia, Spain

Deep Endometriosis, Endometriosis Surgery, Cure Endometriosis, Treat endometriosis
Endometrioma, cystectomy, endometriosis operation
Pre and post-surgical medical treatment in surgery for endometriosis in Valencia, Spain.
Contact the Endometriosis Treatment Specialist
Leave us your information and query to offer you personalized medical advice

Consulta Internacional
If you want remote medical care, you can consult through the following links:
International Appointment
Online Consultation
Whatsapp: + 34 679 112 179